The bottleneck is real. It's in the government's own data.
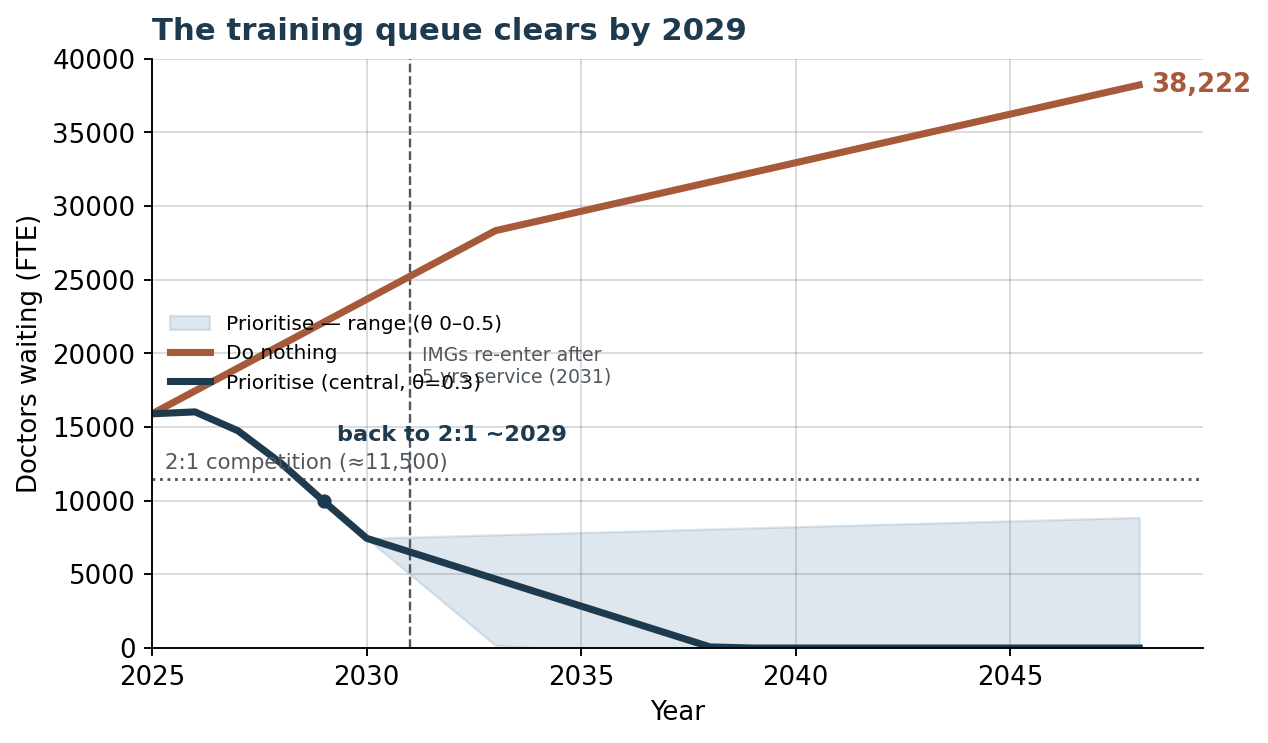
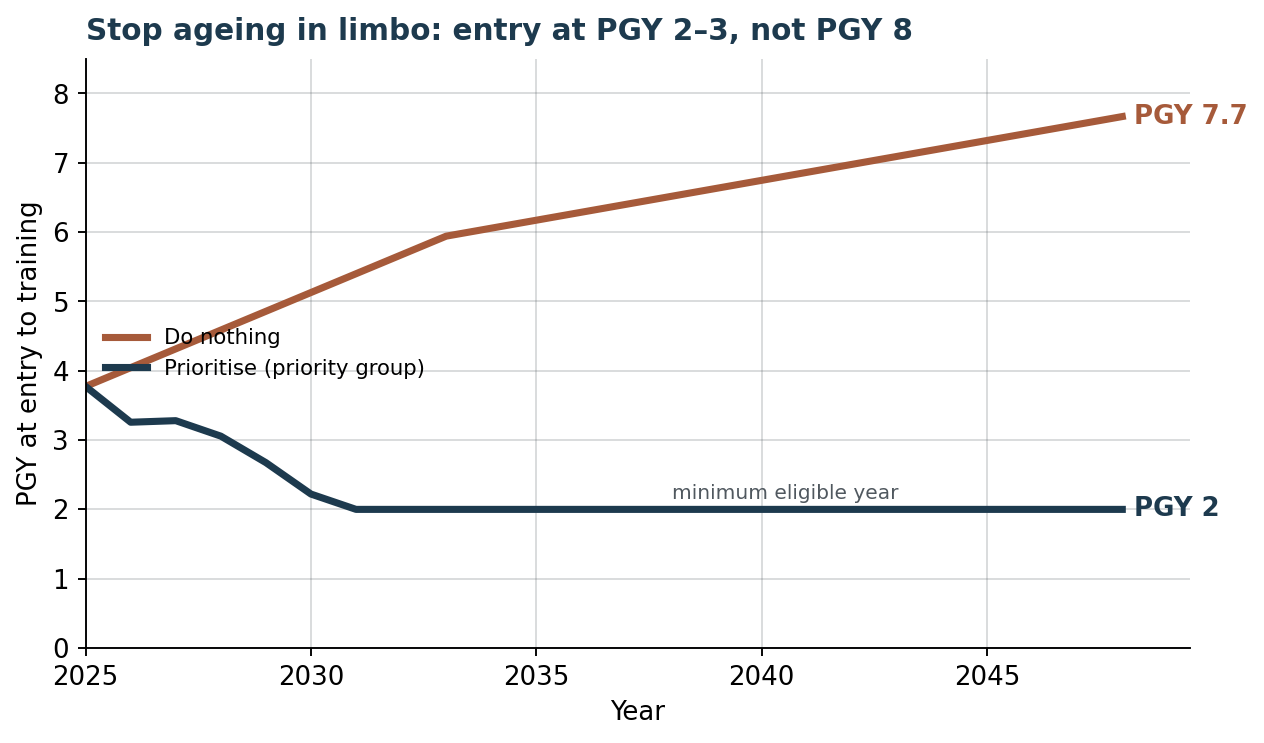
Australia trains more medical students than ever. The number of specialty training places has barely moved. So a growing crowd of fully-qualified junior doctors competes for a near-static number of places. Progression into training has already fallen from 52% a year to 33%. The government's own modelling says it could reach 15% by 2048.
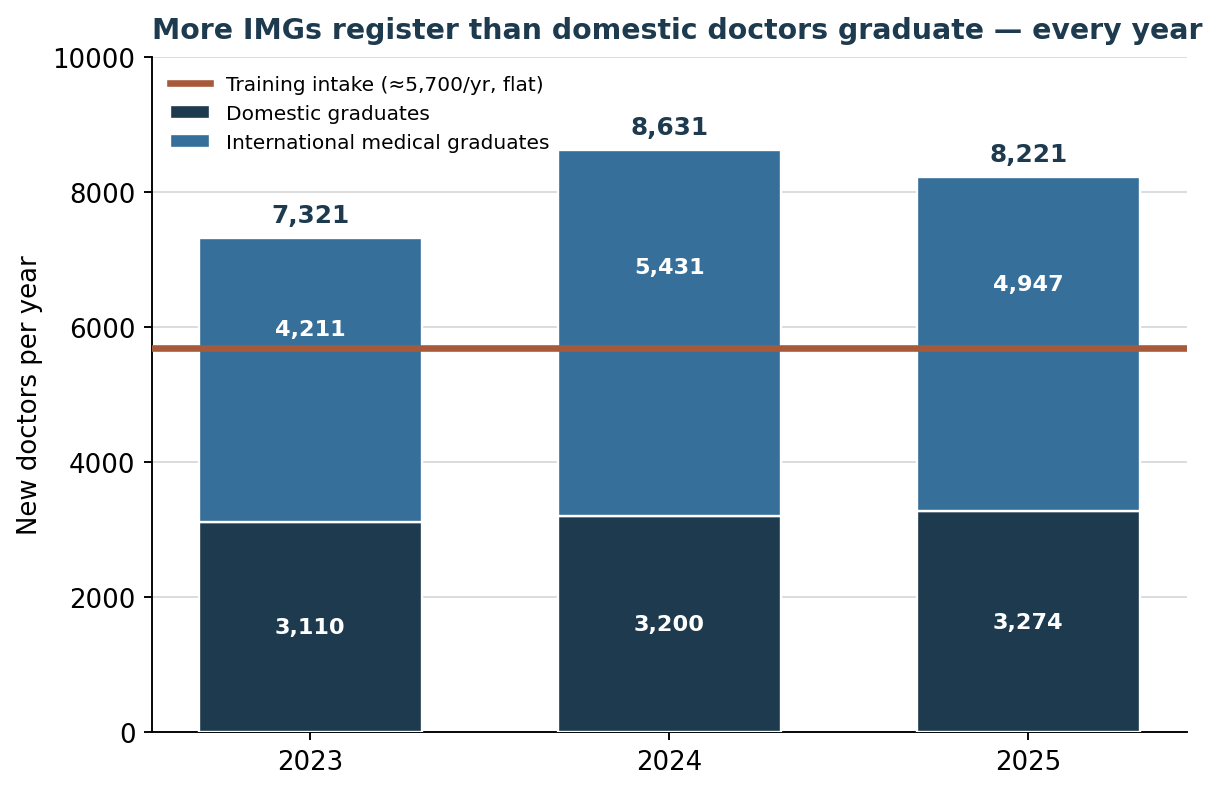
Every year, Australia registers more international medical graduates than it graduates domestic doctors. The number of training places stays flat.
This is not about individual international doctors. They are our colleagues and our friends. Rural Australia depends on them. Our target is a policy choice: a government that recruits past a queue of graduates it already paid to train, instead of building the training places that would let everyone through. The fair fix sends overseas recruitment where it is genuinely needed. It does not punish the doctors already here.